Hypertension
Hypertension is defined as a BP > 140/90mmHg in clinic or > 135/85mmHg with 24hr ABPM/at home
The risk factors for it can be categorised into if they're non-modifiable or modifiable:
Non-modifiable - 65+, FHx, Afro-Caribbean
Modifiable - Obese, Lack of exercise, Smoking, Alcohol, Stress
Usually asymptomatic and diagnosed during regular checks.
Classification
Primary HTN - Most common type (95%), and is when there's no identifiable cause.
Secondary HTN - This is when there's an identifiable cause. The most common cause here is Renal disease (overactivation of the RAAS). The other less common causes include:
Endocrine - Cushing’s (high cortisol), Conns (high aldosterone), Phaeochromocytoma, Acromegaly
Pre-eclampsia
Drugs - Steroids, COCP, NSAIDs
Malignant HTN - Severe, rapid rise in BP > 180/120mmHg leading to end-organ damage. Presents with evidence of end-organ damage e.g. papilloedema, retinal haemorrhages, new confusion, seizure, HF, AKI.
White-coat HTN - High BP during consultations (normal ABPM)
Masked HTN - High BP on ABPM (normal during consultations)
Staging
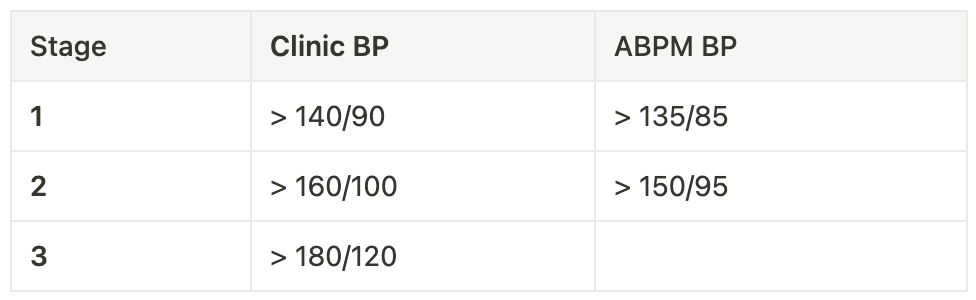
Investigations
If clinic reading > 140/90mmHg, a 24hr ABPM is needed to confirm the diagnosis.
The investigations done are mainly to check for end-organ damage:
Bloods - Glucose, U+E’s, Lipid profile
Urine dip and Albumin:Creatinine Ratio (ACR) - haematuria and proteinuria
Fundoscopy - hypertensive retinopathy
ECG - LV hypertrophy
Management
Lifestyle changes - Smoking cessation, Reduce alcohol and caffeine, Exercise, Diet, Reduce stress
N.B. These lifestyle changes tend to be the only management needed for patients with Stage 1 HTN.
Medication ladder for those < 55 year olds: ACTS
ACEi/ARB
CCB (DHP)
Thiazide diuretic - Thiazide-like diuretics, such as indapamide, are preferred to the conventional drugs like bendroflumethiazide
Spironolactone (use alpha/beta blocker if K > 4.5)
Medication ladder for those > 55 years OR African/Caribbean: CATS
CCB (DHP)
ACEi/ARB
Thiazide diuretic - Thiazide-like diuretics, such as indapamide, are preferred to the conventional drugs like bendroflumethiazide
Spironolactone (use alpha/beta blocker if K > 4.5)
If Diabetic, the patient should be started on an ACEi/ARB (regardless of age/ethnicity).
N.B. ARB can be used instead of ACEi if patient can’t tolerate it e.g. due to cough.

N.B. Young black men have a poor response to ACEi and B-blockers as they are salt-conservers by background, and therefore resistant to renin manipulation.
Complications
Heart:
IHD - Accelerates atherosclerosis in coronary arteries
HF - LV has to work harder against the increased systemic pressure, so undergoes compensatory hypertrophy. Eventually, the hypertrophied LV decompensates and fails → Left HF
Brain:
Stroke - Accelerates atherosclerosis
Haemorrhage - Rupture of tiny berry aneurysms → SAH
Vascular Dementia
Kidney:
CKD - Hypertensive nephropathy - Progressive arteriosclerosis in renal arteries, causing renal ischaemia = Tubular atrophy, Interstitial Fibrosis, and Glomerular sclerosis. USS will show small, fibrotic kidneys.
Eye:
Hypertensive Retinopathy - Flame haemorrhages, cotton-wool spots, yellow hard exudates, and papilloedema