Cranial Nerve Palsies
Optic Neuritis
There are 2 types of it:
Retrobulbar neuritis (inflammation behind eye) – Most common - Optic head looks normal
Papillitis (inflammation of optic head) – Optic head looks inflamed
Presentation - Pain w/movement, visual loss, impaired colour vision, Marcus-Gunn Pupil (RAPD)
Investigations:
Screening tests - ANA, ANCA, ESR, Immunoglobulins, Syphilis, HIV
MRI Brain and orbits w/contrast
Visual evoked potentials
Anti-aquaporin4 if bilateral presentation - it indicates Neuromyelitis optica, which is often confused with MS
Management - 5 days 500mg PO Methylprednisolone

CN 3 (Oculomotor) Palsy
This nerve is composed of deep, extraocular muscle somatic efferents, and superficial parasympathetic efferents. It can be affected in 2 different ways:
Medical e.g. ischaemia or diabetes - The deep, somatic efferents are mainly affected, therefore it's pupil-sparing
Surgical e.g. aneurysms or trauma - Superficial parasympathetics are mainly affected, therefore it's non-pupil sparing
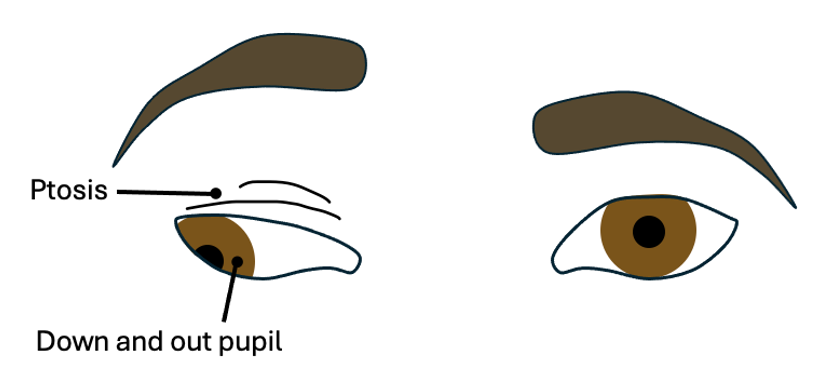
Presentation - Ptosis, Down and out pupil
The most common causes of a surgical palsy is a PCOM aneurysm (posterior communicating artery), and Cavernous sinus thrombosis.
N.B. Cavernous sinus thrombosis would also present with palsies of CNs 4, 5 (v1, 2), and 6.

CN 4 (Trochlear) Palsy
Presentation:
Unable to turn down and inwards (towards nose)
Double vision
To get around this defect, patients may tilt their head to the side opposite the affected eye to compensate and avoid double vision = Ocular torticollis.

CN 6 (Abducens) Palsy
Presentation:
Unable to move affected eye out laterally
May result in double vision

CN 7 (Facial) Palsy
Can either be due to an UMN or LMN cause, which present slightly differently:
UMN type - Presents with Incomplete weakness (More subtle), Forehead and eye sparing, Brisk jaw reflex
LMN type aka Bell's Palsy - Complete weakness, Not Forehead-sparing (Unable to lift eyebrow), Weak eye closure

Bell’s palsy will also present with dry eyes, altered taste sensation, and hyperacusis. Treated with 50-60mg Prednisolone. The main complication with this is corneal ulceration (sclera constantly exposed to air, therefore at risk of ulceration), so the patient may need artificial tear drops.
Ramsay-Hunt syndrome occurs when VZV (Shingles) affects CN7, causing severe ear pain, a vestibular rash, taste dysfunction, and hyperacusis. Treated with Aciclovir, steroids, and analgesia.
If the rash involves the tip of the nose, it's called a positive Hutchinson's sign (worrying sign). This indicates that the virus has affected the nasocilliary nerve, which also innervates the eye, therefore could lead to vision loss if left untreated.

Signs of CN7 and CN8 palsies indicate a problem at the Cerebellopontine angle, which can be caused by an Acoustic neuroma (aka vestibular shwanomma).

Important Links:
https://bestpractice.bmj.com/topics/en-gb/966
https://bestpractice.bmj.com/topics/en-gb/773
“Vestibular schwannoma” © RadsWiki CC BY-SA 3.0 (https://creativecommons.org/licenses/by-sa/3.0/)